M. G. White1, M. K. Applewhite1, B. C. James1, H. Safiuddin1, L. Abdulrasool1, H. Jamil1, E. L. Kaplan1, P. Angelos1, R. H. Grogan1 1University Of Chicago,Endocrine Surgery Research Group, Department Of Surgery,Chicago, IL, USA
Introduction: The use of energy devices in surgical procedures has become common after the introduction of bipolar and ultrasonic energy devices in the late 1990s. Recently, integrated laparoscopic devices, which simultaneously combine bipolar and ultrasonic energies, has resulted in increased interest in this technology for open surgery. This study was performed to quantitatively compare heat transfer and collateral tissue damage that may be associated with these devices.
Methods: Three serial firings for each setting of the bipolar (Ligasure Small Jaw), ultrasonic (Harmonic Focus), and integrated (Thunderbeat Open Fine Jaw) devices were applied in vivo to various porcine tissue types including: liver, muscle, and thyroid. Thermocouplers were inserted into surrounding tissue at 1 mm intervals to measure temperatures over time as the devices were fired. Temperature was reported in degrees Celsius. Recurrent laryngeal nerve (RLN) monitoring was performed to determine the practical implications of the heat generation in tissue. This was done with firings of each device at successively decreasing distances from the RLN until signal was lost. Statistical analysis included t-tests and ANOVA was performed using STATA.
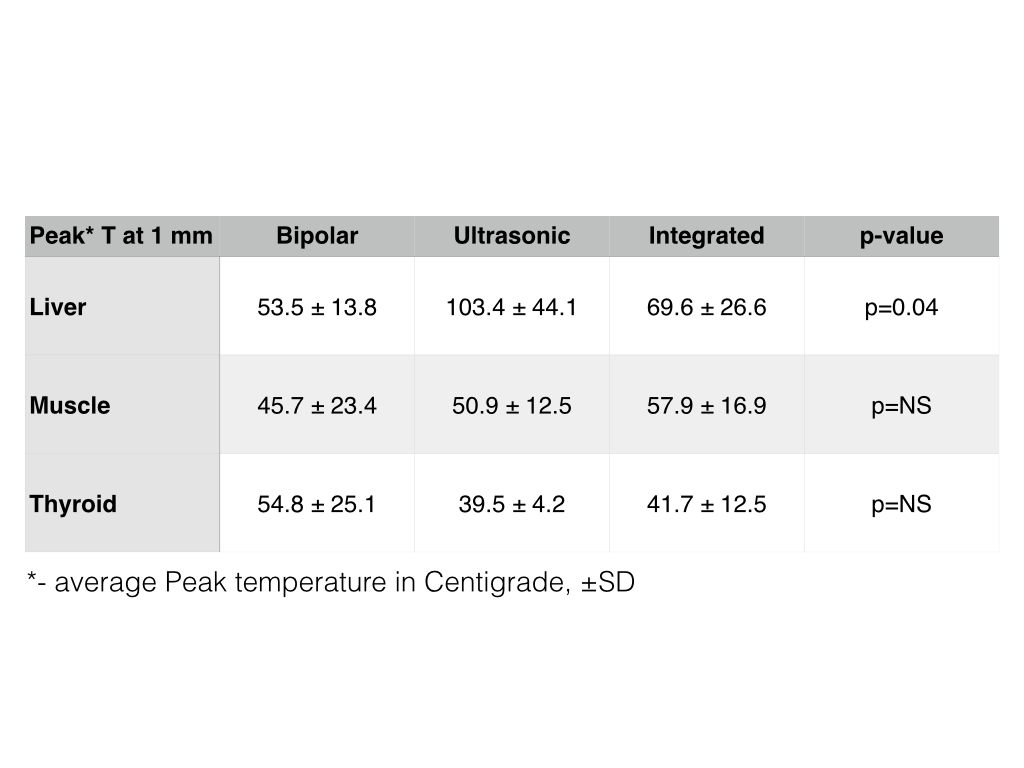
Results: The amount of heat generated in the tissue between the lowest and highest settings was similar for each device tested (p=0.11-0.81). However, when comparing heat generated across these devices for the peak temperature reached at 1 mm, the peak temperature recorded in liver tissue was observed with HF (103.4 ± 44.1), in muscle tissue – with OFJ (57.9 ± 16.9); and in thyroid – with LS (54.8 ± 25.1). RLN signal was lost after firing 1mm away from the RLN for all devices while nerve monitor signal was not affected by firing at ≥2 mm.
Conclusion: Comparable quantitative data on heat dispersion and collateral tissue damage by surgical energy devices is one of the important factors that surgeons use to make informed decisions regarding the devices they choose for surgery. Our findings conclude that heat transfer as a function of depth was similar among all three devices with the exception of HF resulting in significantly higher temperatures than OFJ and LS in the liver. Liver tissue showed the most consistent results between experiments therefore we recommend that liver tissue be used for any future experiments on heat transfer to tissue. Although collateral heat transfer is an important consideration, tissue cutting speed and dissection capability are also key factors when choosing a surgical device for clinical applications. Further studies are required to evaluate all relevant performance attributes in a controlled clinical environment.