A. Hassan1, P. Rhee1, A. A. Haider1, N. Kulvatunyou1, T. O’Keeffe1, A. Tang1, R. Latifi1, G. Vercruysse1, D. Green1, F. Randall1, B. Joseph1 1The University Of Arizona,Trauma,TUCSON, ARIZONA, USA
Introduction:
The optimal management of bowel injury in the setting of damage control laparotomy (DCL) is not well defined. The aim of this study was to compare primary anastomosis (PA) versus bowel discontinuity (BD) in DCL at the first operation.
Methods:
An 8-year (2006-2013) retrospective analysis of all patients undergoing trauma laparotomy at our Level 1 trauma center was performed. We included patients with DCL requiring bowel resection. We divided the patients into two groups based on their treatment: PA and BD. Patients in BD group were re-anastomosed during the second operation. Outcome measures were mortality and complications. We compared the two groups for differences in demographics, injury parameters, lab data and outcomes.
Results:
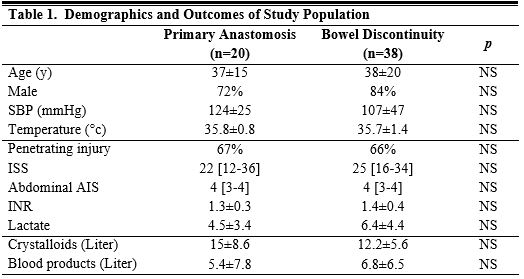
A total of 162 patients had DCL during the study period of which 58 patients (36%) were included in our analysis. 32% (n=20) of the patients had a PA while the remaining 68% (n=38) patients had BD. Overall mortality rate was 34%. There was no difference in patient characteristics and intra-abdominal organ injuries between the two groups (Table 1). On multivariate analysis patients with BD had 4.6 times higher mortality rate compared to patients with PA (OR (95%CI) = 4.6 (1.08-25); p=0.04).
Conclusion:
Patients left in bowel discontinuity had 5 times higher risk of mortality compared to patient undergoing a primary anastomosis. Iatrogenic bowel obstruction after damage control laparotomy may have physiological effects contributing to adverse outcomes.