Y. Kim1, F. Gani1, F. Bagante1, G. A. Margonis1, D. Wagner1, L. Xu1, S. Buttner1, J. O. Wasey2, S. M. Frank2, T. M. Pawlik1 1Johns Hopkins University School Of Medicine,Surgery,Baltimore, MD, USA 2Johns Hopkins University School Of Medicine,Anesthesiology And Critical Care Medicine,Baltimore, MD, USA
Introduction: Stratifying a patient’s risk for perioperative packed red blood cell (PRBC) transfusion when planning major abdominal surgery is of interest to both patients and providers. We sought to identify preoperative factors associated with receipt of PRBC to create a nomogram that predicts an individual’s risk of transfusion with major abdominal surgery.
Methods: A nomogram to predict receipt of perioperative transfusion was constructed using a cohort of patients who underwent hepato-pancreatico-biliary (HPB)(n=2,792) and colorectal (n=2,171) surgery between 2009-2014. Discrimination and calibration of the nomogram was tested using area-under-the-curve (AUC) receiving operator curves and calibration plots.
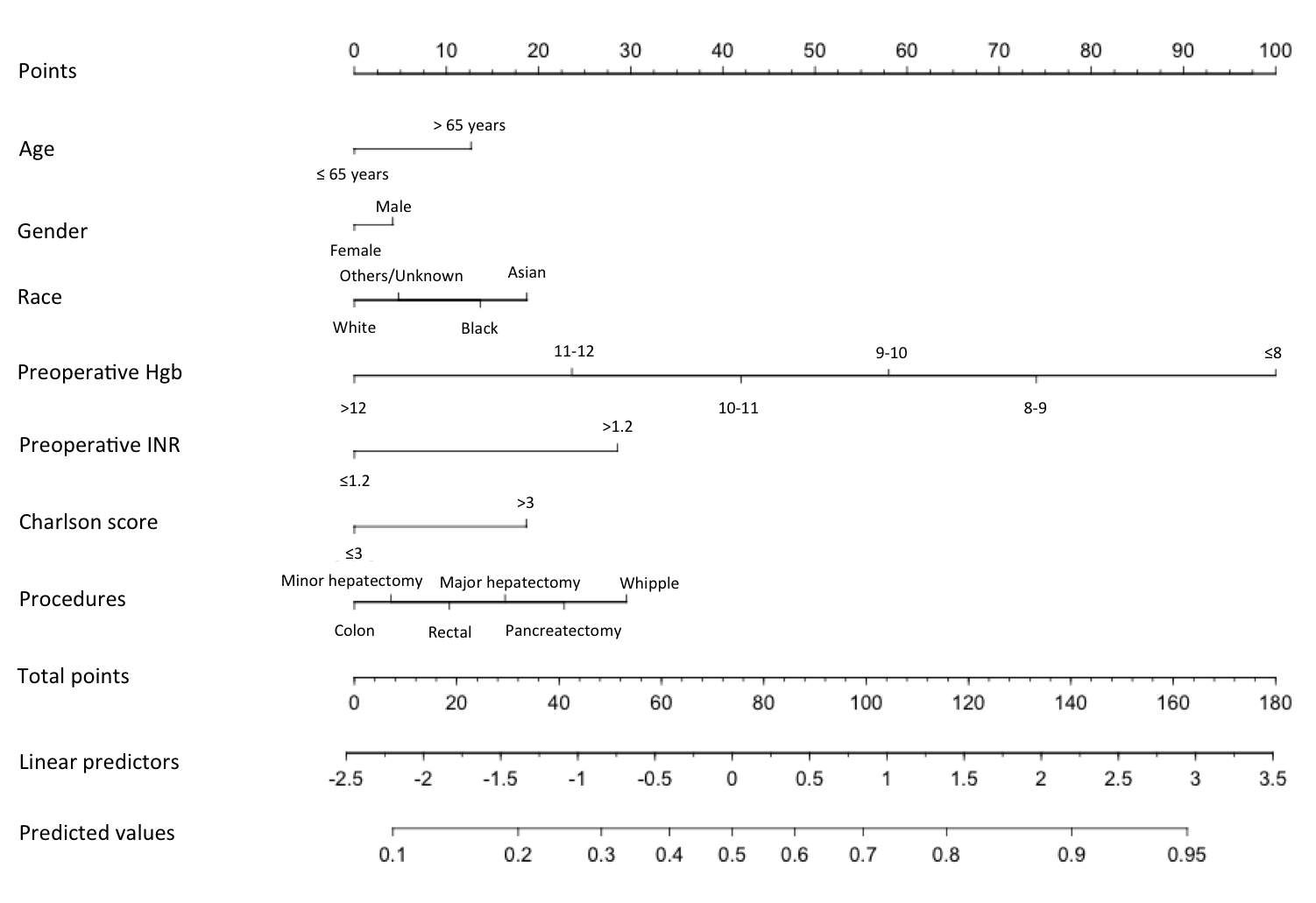
Results: Among 4,963 patients undergoing either a HPB (56.3%) or colorectal (43.7%) procedure, 1,549 received ≥1 unit of PRBC for a perioperative transfusion rate of 33.1%. On multivariable analysis, age ≥65years (OR=1.5), race (Black: OR=1.6, Asian: OR=1.9), male sex (OR=1.1), preoperative Hb ≤8g/dL (vs. >12g/dL: OR=27.5), preoperative INR>1.2 (OR=2.6), Charlson score>3 (OR=1.9), and procedure type (colon surgery, referent: minor hepatectomy OR=1.1, rectal surgery OR=1.4, major hepatectomy OR=1.7, distal pancreatectomy OR=2.1, whipple procedure OR=2.7) were associated with risk of transfusion (all P<0.05). A nomogram was constructed to predict receipt of transfusion using these variables (Figure). Discrimination and calibration of the nomogram revealed good predictive abilities (AUC 0.76). Bootstrap validation of model accuracy revealed minimal evidence of model overfit.
Conclusion: Independent preoperative variables were used to create a nomogram to predict the likelihood of PRBC transfusion. This nomogram may be useful in stratifying a patient’s risk of needing a blood transfusion around the time of major abdominal surgery.