N. Valsangkar1, P. J. Martin1, J. S. Mayo1, D. V. Feliciano1, T. A. Zimmers1, L. G. Koniaris1 1Indiana University School Of Medicine,Department Of Surgery,Indianapolis, IN, USA
Introduction: The value of subspecialty surgical fellowships is unclear. Fellows might compete with residents for advanced clinical activities but potentially enhance research and clinical excellence within subspecialties. Evidence for the latter was unavailable. Herein we sought to determine the impact of post-residency fellowships on academic output including NIH funding rates in departments of surgery.
Methods: Fellowships offered at the top 55 NIH-funded departments of surgery were identified. Publications, citations and NIH funding history were determined for 4,015 faculty. Mann-Whitney-U test and t-test were used as appropriate.
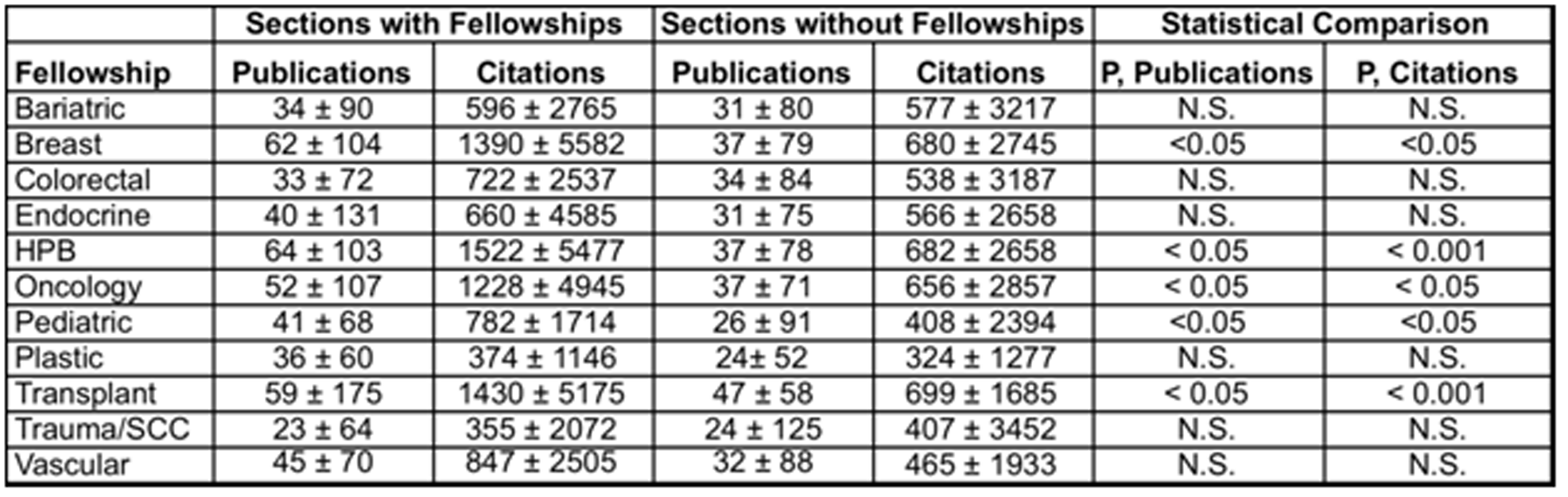
Results: Cardiothoracic surgery fellowships (CT) were offered at all departments. Other surgical fellowships are offered in 52 of 55 departments (96.4%). Median department publications/citations (P/C) increased with the number of fellowships offered in addition to CT: no fellowship (27±93/437±2509), 1-3 fellowships (34±90/559±3046) and 4 or more (40±97/716±3200, p<0.05). No change in sectional P/C was noted for post-residency bariatric-MIS, colorectal, endocrine, plastic, trauma/CCS/ACS or vascular fellowships. Significant sectional improvements in P/C were observed for breast, HPB, oncology, pediatric, and transplantation (50%-75% increase in P/C versus institutions without fellowships, p<0.05). No differences in divisional or departmental NIH funding rates were observed regardless of the type or number of fellowships offered.
Conclusion: Select fellowships appear to improve the P/C for their respective subspecialty sections. Fellowships have no impact on NIH funding rates. These data suggest that better research is not occurring at many institutions that are producing subspecialists and that clinical training of fellows preempts academic productivity in many subspecialties.