C. D. Tzeng1, B. M. Evers1, J. B. Zwischenberger1, M. V. Williams1, B. R. Boulanger1, P. C. McGrath1, J. T. Martin1 1University Of Kentucky,Lexington, KY, USA
Introduction:
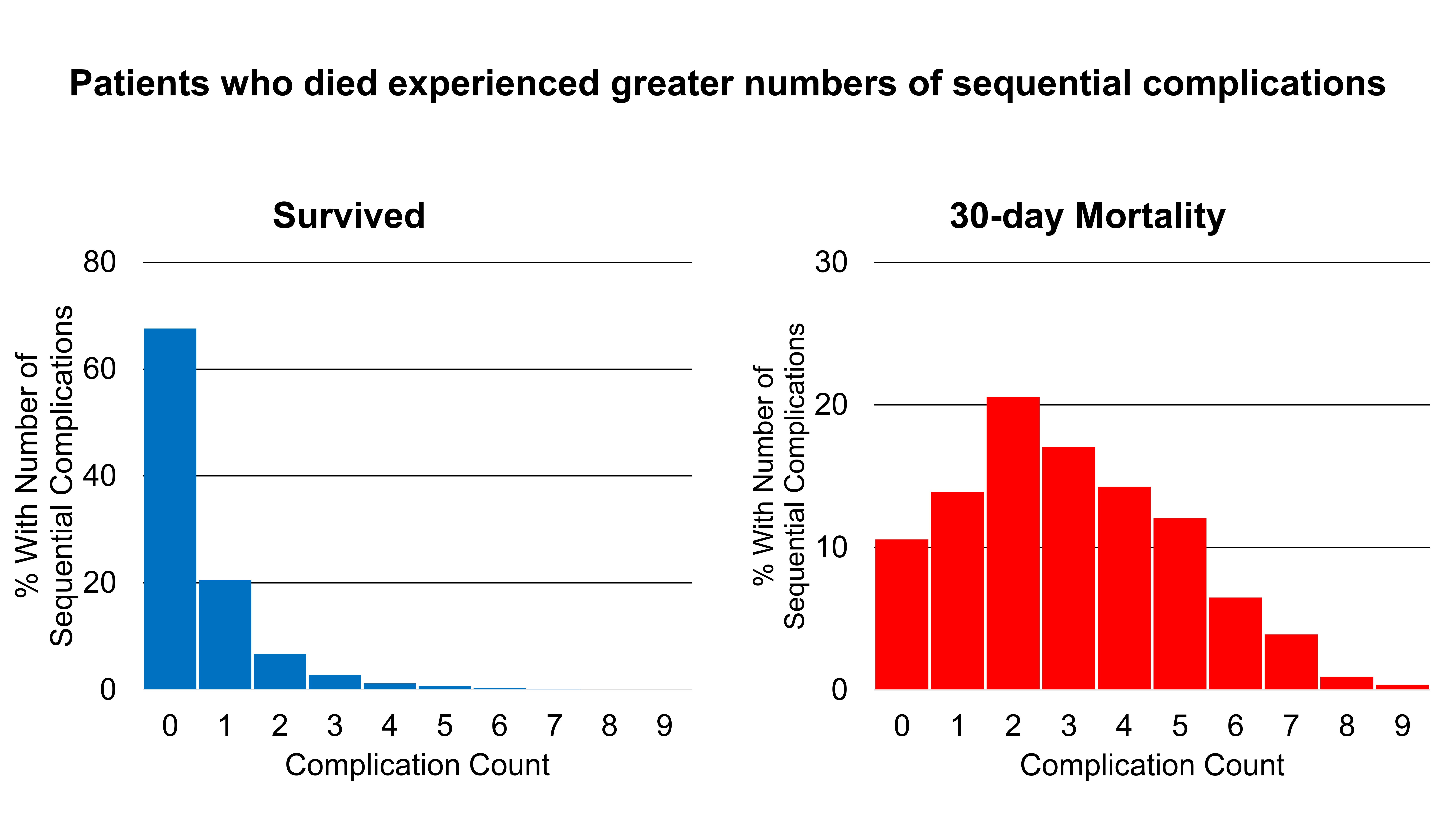
Failure to rescue (FTR: % patients who died after ≥1 complication) is an increasingly important hospital performance measure. This study sought to analyze 6 high-risk index operations to identify the most common complication cascades and their initial physiologic insults which could be targeted to prevent FTR.
Methods:
Elective patients with hematocrit ≥30% undergoing 6 index procedures were identified from the 2012-2013 ACS-NSQIP dataset. Association between number of morbidity events and FTR was analyzed with logistic regression. The most common complication cascade was analyzed for each procedure to identify the most common initial complication and to compare FTR rates.
Results:
34,556 patients underwent esophagectomy (morbidity/mortality/FTR-32.8%/2.1%/5.5%), lung resection (14.1%/1.7%/9.7%), gastrectomy (16.9%/1.7%/9.2%), pancreaticoduodenectomy (25.8%/2.3%/7.8%), hepatectomy (15.5%/1.6%/9.8%), and colectomy (15%/1.3%/6.5%). Patients who died suffered more sequential complications (Figure) and multiplicative odds of death with additional events. Bleeding requiring transfusion was the most common initial event in every index procedure (13.6%-overall, range 8.1%-lung, 21.5%-pancreaticoduodenectomy/hepatectomy). Among deaths, the most common cascade was bleeding (42%), respiratory failure (18%), septic shock (28%). Among non-transfused patients, the most common cascade was superficial infection, organ space infection, sepsis. Non-transfused patients were less likely to have multiple complications and had better mortality and FTR rates (mortality 0.99% vs. 4.84%; FTR 5.37% vs. 11.99%, p<0.001).
Conclusion:
Avoidance of perioperative transfusions mitigates the magnitude of complication cascades and improves FTR rates. Although bleeding requiring transfusion is commonly overlooked when measuring perioperative complications, it is the most common sentinel domino to fall. To augment surgical mortality reduction programs, hospitals should pursue aggressive programmatic transfusion avoidance strategies in the perioperative setting.