C. E. Cauley1, G. Anderson1, M. E. Menendez3, B. Bateman2, K. Ladha2, A. B. Haynes1 1Massachusetts General Hospital,Department Of Surgery,Boston, MA, USA 2Massachusetts General Hospital,Department Of Anesthesiology,Boston, MA, USA 3Massachusetts General Hospital,Department Of Orthopedic Surgery,Boston, MA, USA
Introduction:
In 2000 the Joint Commission recommended using pain as a 5th vital sign, increasing focus on postoperative pain control. However, the benefits of pain management must be weighed against the potentially lethal risk of postoperative opioid overdose (POOD). This analysis aims to 1) describe national trends and outcomes of in-hospital POOD in patients undergoing surgery and 2) identify predictors of POOD.
Methods:
This is a retrospective multi-institutional cohort study of patients undergoing a major elective operation from 2002 to 2011 in the Nationwide Inpatient Sample. Patients with POOD were identified using ICD-9 codes for poisoning from or adverse effects of opioids. Patients with adverse effects from opioids required a concurrent code for respiratory failure, apnea, or hypoxia to be included in the POOD cohort. Multivariate logistic regression was used to identify predictors of POOD.
Results:
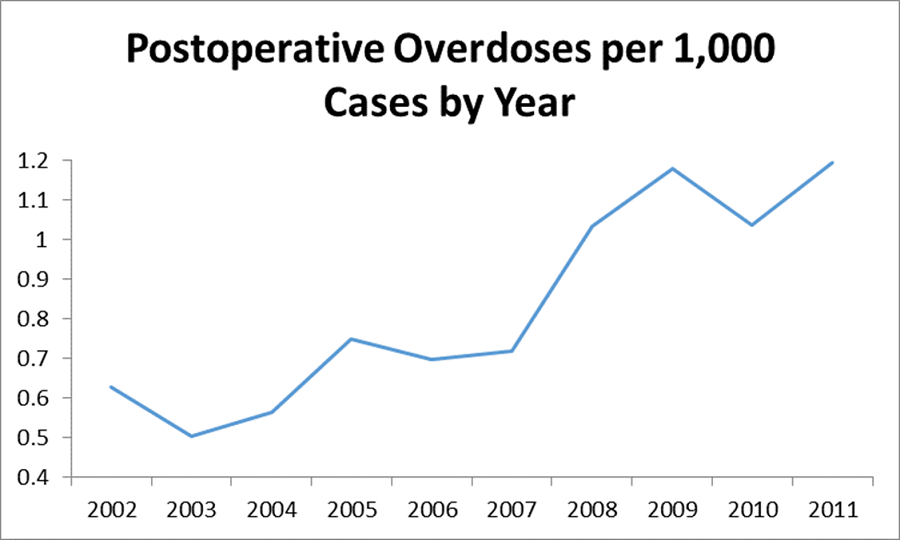
Among 13,982,557 patients, 11,669 (0.083%) had POOD with the rate increasing over the study period from 0.6 to 1.2 per 1,000 cases. Patients with POOD died more frequently during hospitalization (1.7% vs. 0.47%, p-value=<0.001). Substance abuse history was the strongest predictor of POOD (OR=14.9; 95% CI: 12.5-17.6) on multivariate analysis. Gender, age, race, income, geographic location, operation type, and comorbid diseases were significant predictors of POOD. Hospital variables including teaching status, size, and urban/rural location did not predict POOD.
Conclusion:
POOD is a rare, but potentially lethal complication, with increasing prevalence. Perioperative care providers should consider predictors of POOD to identify patients at greatest risk, while providing adequate pain control. Postoperative monitoring and treatment protocols should be thoughtfully employed to target high risk patients and avoid this potentially fatal complication.