K. B. Savoie1,2, F. Thomas2, S. S. Nouer3, E. Y. Huang1 1University Of Tennessee Health Science Center,Surgery,Memphis, TN, USA 2University Of Tennessee Health Science Center,Biostatistics & Epidemiology,Memphis, TN, USA 3University Of Tennessee Health Science Center,Preventive Medicine,Memphis, TN, USA
Introduction: Intussusception, the most common cause of bowel obstruction in infants and neonates, is less common in children older than 3 years. Standard of care for children less than 3 years is fluoroscopic enema reduction (FER). Use of FER in older children, especially children older than 6 years, is controversial. We utilized the Pediatric Health Information System (PHIS) database to determine whether older children are at higher risk for operative intervention and other morbidities, such that fluoroscopic reduction should not be attempted.
Methods: The PHIS database was reviewed from 1/1/2009-6/30/2014. Patients with chronic medical conditions, including Peutz-Jegher Disease and Henoch-Schonlien Purpura, were excluded. Individual patients were followed across admissions for 6-months from initial presentation or until bowel resection occurred. Successful FER was defined as having had radiologic reduction without subsequent surgery for 6 months.
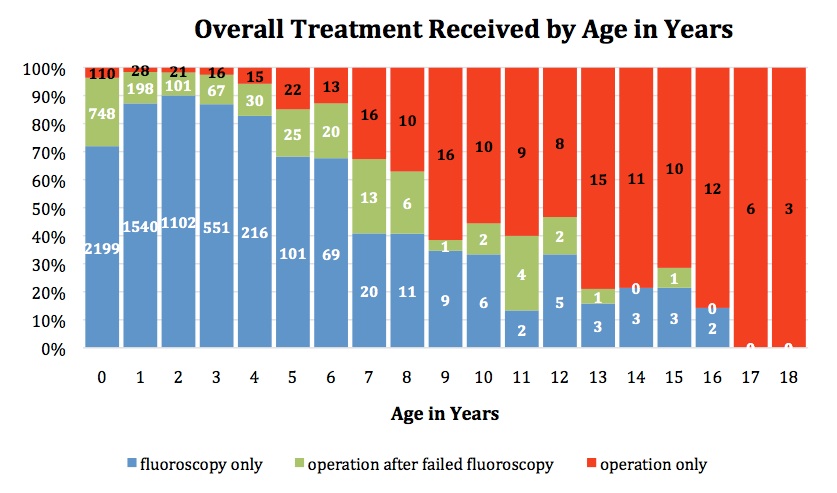
Results: 7412 patients were identified. 6681 were ≤3 years. Of these, 175 (2.6%) underwent primary surgery, 1114 (16.7%) had surgery at some point after FER, and 5392 (80.7%) were successfully treated with FER. 731 patients were > 3 years: 176 (24.1%) underwent primary surgery, 105 (14.4%) had surgery after FER, and 450 (61.6%) were successfully treated with FER. In patients >3 years, length of stay (LOS) between patients who underwent primary surgery versus those who underwent surgery after FER at their initial visit was similar (Median 4 days vs 4 days, p = 0.06); those undergoing successful FER had a median LOS of 1 day (p <0.0001). The frequency of patients with a concurrent discharge diagnosis within a tumor category were similar in patients ≤3 years and patients >3 years (4.8% vs 6.3%, p = 0.07). The frequency of Meckel’s diverticulum was 2.3% in those ≤3 years and 13.5% in those >3 years (p <0.0001). There were only 3 patients who died; all were ≤3 years. In those failing FER and undergoing surgery, there was no difference in LOS between those ≤3 and >3 years (Median 3 vs 4 days, p = 0.09); <1% of older children were admitted to the intensive care unit as compared to 9.8% in those ≤3 years (p <0.01). Older age was not associated with increased risk of recurrent admission for intussusception (p = 0.58).
Conclusion: Although older children with intussusception were more likely to undergo operative intervention than younger children, PHIS data analysis suggests that fluoroscopy may be a safe initial procedure for a majority of older children. A prospective observational trial would be necessary to confirm this finding, which could help inform future treatment algorithm for older pediatric patients presenting with intussusception.