E. A. Busch2, S. Koller2, M. M. Philp2, H. Ross2, H. A. Pitt1,2 1Temple University,Temple University Health System,Philadelpha, PA, USA 2Temple University,Temple University School Of Medicine,Philadelpha, PA, USA
Introduction: Frailty has been documented to adversely influence the outcomes of colorectal surgery. The potential role that the indication for surgery may have on morbidity and mortality has not been adequately studied. In addition, the interplay between frailty and indication has not been explored. Thus, the aim of this analysis was to define the influence that patient frailty and surgical indication have on the outcomes of colorectal surgery.
Methods: The American College of Surgeons- National Surgical Quality Improvement Program (ACS-NSQIP) Participant Use Files were queried for patients undergoing colorectal surgery in 2012 and 2013. Frailty was defined as five or more of eight preoperative variables including functional status, ASA 4 or 5, hypoalbuminemia, heart failure, COPD, diabetes mellitus, hypertension and male gender. Ten surgical indications included acute or chronic diverticulitis, bleeding, cancer without or with obstruction, IBD (Crohn’s or ulcerative colitis) enterocolitis, benign polyps or volvulus. Overall morbidity, serious morbidity and 30-day mortality were defined by ACS-NSQIP. Other known risk factors including age, BMI, race, emergent surgery and operative approach also were analyzed. Univariate analyses and multivariable logistic regression were performed in STATA 13.1.
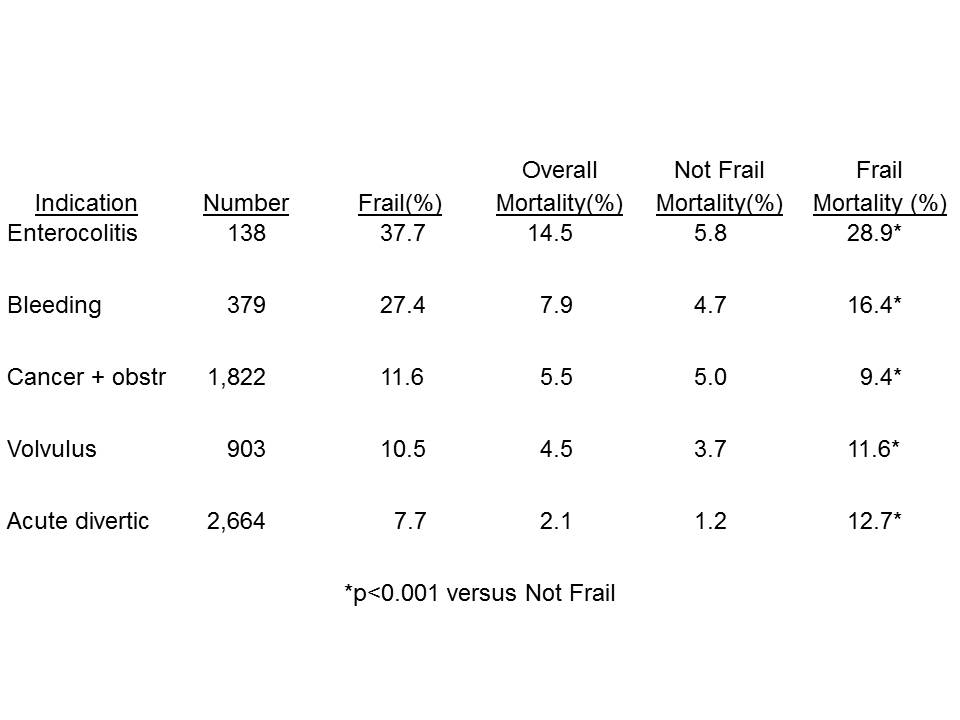
Results:Of 29,219 patients undergoing colectomy, 2,077 (7.1%) were frail. The incidence of frailty varied from 1% for 1,994 Crohn’s patients to 38% among 138 patients with enterocolitis. Frailty increased mortality (p <0.05) for every indication except Crohn’s disease as well as serious morbidity (p<0.05) for all indicators except Crohn’s and benign polyps. The interplay between frailty and indication in the five groups with the worst mortality outcomes is presented in the Table.
In multivariable analyses both frailty (Odds Ratios 1.57-2.98) and surgical indication (Odds Ratios 1.11-1.47) remained independent predictors of overall morbidity, serious morbidity and mortality (all p<0.01).
Conclusion:The incidence of frailty varies dramatically among the multiple indications for colectomy. Both patient frailty and surgical indication influence the outcomes of colorectal surgery.