J. K. Horwitz1, D. T. Huynh1, T. F. Barrett1, V. S. Tung1, C. M. Divino1 1Mount Sinai School Of Medicine,Department Of Surgery,New York, NY, USA
Introduction: An anastomotic leak (AL) is a serious complication of gastrointestinal surgery. Once identified, anastomotic leaks may be definitively managed with percutaneous drainage or re-exploration. The aim of our study is to compare CT imaging versus diagnostic laparoscopy (DL) as initial management strategies for evaluating patients with clinically suspected anastomotic leaks.
Methods: Patients who developed an AL at The Mount Sinai Hospital from 2003-2015 were identified retrospectively. Patients who were managed with an exploratory laparotomy without a prior CT or DL were excluded. The remaining patients were stratified into two groups based on the initial management of the suspected AL, CT versus DL. The sensitivities of the two diagnostics were compared as well as the outcomes, including: length of stay (LOS), SICU admission/LOS, 30-day mortality, requirement for a 2nd reoperation, and readmission. The groups were compared using the Fisher’s exact test and χ2 for categorical variables and the Mann-Whitney-Wilcoxon test for continuous variables.
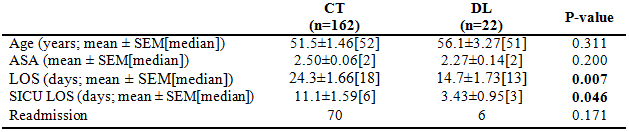
Results: 184 patients who suffered ALs and met our inclusion criteria were identified. Within this group, 162 initially received a CT while 22 directly underwent a diagnostic laparoscopy. No differences were found between the groups’ age, sex, ASA, BMI, or comorbidities. The sensitivities of CT and DL were found to be 52.5% and 72.7%, respectively. No differences were found between the groups’ SICU admission rates, 30-day mortality, requirement for a 2nd reoperation, or readmission. A significant difference in LOS was observed between the two groups (p=0.007) with a median LOS of 18 days and 13 days for CT and DL, respectively. SICU LOS was also found to be significantly longer in the CT group (p=0.046) with a median SICU LOS of 6 and 3 days for CT and DL, respectively.
Conclusion: Suspected ALs must be approached with urgent and decisive action. Our data supports diagnostic laparoscopy as an effective and safe initial approach to clinically suspected anastomotic leaks, as demonstrated by a higher sensitivity and shorter LOS relative to CT imaging.