A. Asban1, M. Traa1, N. Melnitchouk2 1Tufts Medical Center,Colorectal Surgery,Boston, MA, USA 2Brigham And Women’s Hospital,Boston, MA, USA
Introduction:
Due to the increase in the successful rate of heart transplant surgery as well as dramatic improvement of immunosuppression medications, the risk and complications of a abdominal and colorectal surgery were poorly described in literature.
Methods:
This is a single institution study of 32 heart transplant recipients who underwent abdominal, including colorectal, operations at Tufts Medical Center between 2003 and 2013. Medical records were reviewed for comorbidities, immunosuppression status, duration post-transplant, type of surgery, type of anesthesia, intraoperative complications, estimated blood loss, postoperative complications, length of stay, readmission and reason of readmission and 30-day mortality rate.
Results:
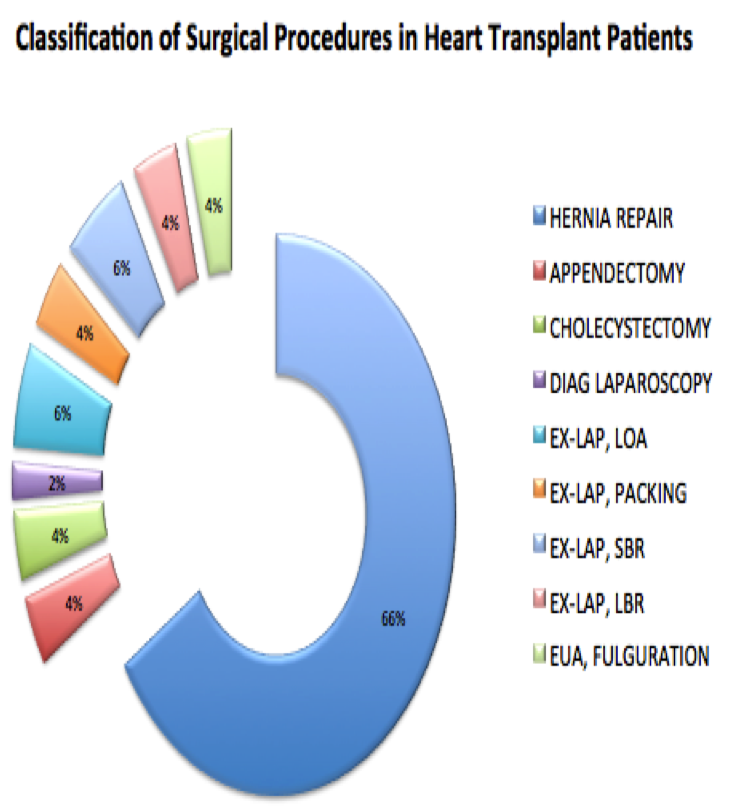
Over the 11-year study period, 32 patients with heart transplant at Tufts Medical Center underwent a total of 50 colorectal (20%) and other abdominal (80%) operations. Colorectal operations included left colectomy, exploratory laparotomy with lysis of adhesion, small bowel resection and examination under anesthesia and fulguration of anal condyloma. The most common procedure overall were incision hernia (40%) and diaphragmatic hernia (18%). 74% of the surgeries were elective and 26% emergencies. 94% of cases were performed under general anesthesia. The study population was 87.5 male and 12.5% female wit mean age of 55 years. In 50% of patients the indication for heart transplant was ischemic heart disease. 58% of patients had undergone abdominal surgery previously, 100% of patients were on immunosuppression, and 46% were on steroids. The median time elapsed since transplant was 765 days (range 1-3,563 days). Intraoperative complications were limited to bleeding (2%) and hypotension (2%). Postoperative complications included deep surgical site infection (4%) and superficial surgical site infection (2%), none of which happened in the colorectal surgery group. Of the bowel resection with anastomoses there were no anastomotic leaks reported. There were no major cardiac events noted in the perioperative period although sinus tachycardia was common intraoperatively. The mean length of stay was 4 days, with an 8% readmission rate for post operative surgical causes (including management of surgical site infection or pneumonia). Thirty-day mortality rate was 0%
Conclusion:
Our experience suggests that abdominal and colorectal surgery in heart transplant recipients is relatively safe. The incidence of surgical site infections was comparable to the general population, and there were no anastomotic leaks in our small sample despite immunosuppression. Surgeons should evaluate heart transplant patients for abdominal and colorectal surgery as they would any other patient presenting for emergency or elective care.