A. A. Hildebrandt1, L. R. Putnam1,2, M. B. Diffley1, K. M. Caldwell1, S. E. Covey1, A. N. Mizenmayer1, K. T. Anderson1,2, A. L. Kawaguchi1,2, L. S. Kao3, K. P. Lally1,2, K. Tsao1,2 1University Of Texas Health Science Center At Houston,Pediatric Surgery,Houston, TX, USA 2Children’s Memorial Hermann Hospital,Pediatric Surgery,Houston, TX, USA 3University Of Texas Health Science Center At Houston,General Surgery,Houston, TX, USA
Introduction: Three-phase (pre-induction, pre-incision, debriefing) surgical safety checklists (SSC) have been widely adopted as an effective tool for decreasing postoperative morbidity and mortality. However, checklist effectiveness has recently been questioned. We aimed to identify potential flaws in the execution of a local, stakeholder-derived SSC, which could lead to its ineffectiveness.
Methods: From May to July 2015, five trained observers directly observed the completion of 11 pre-induction, 19 pre-incision, and 9 debriefing checkpoints during the three-phase SSC for pediatric operations. All checkpoints were assessed for adherence (checking the box). Of the 19 pre-incision checkpoints, 10 were assessed for high fidelity performance (meaningful completion). These fidelity checkpoints represent complex measurable tasks relying on a high-level of team cohesion and communication for meaningful completion. Inter-rater reliability and chi-squared tests were performed; p-values <0.05 were considered significant.
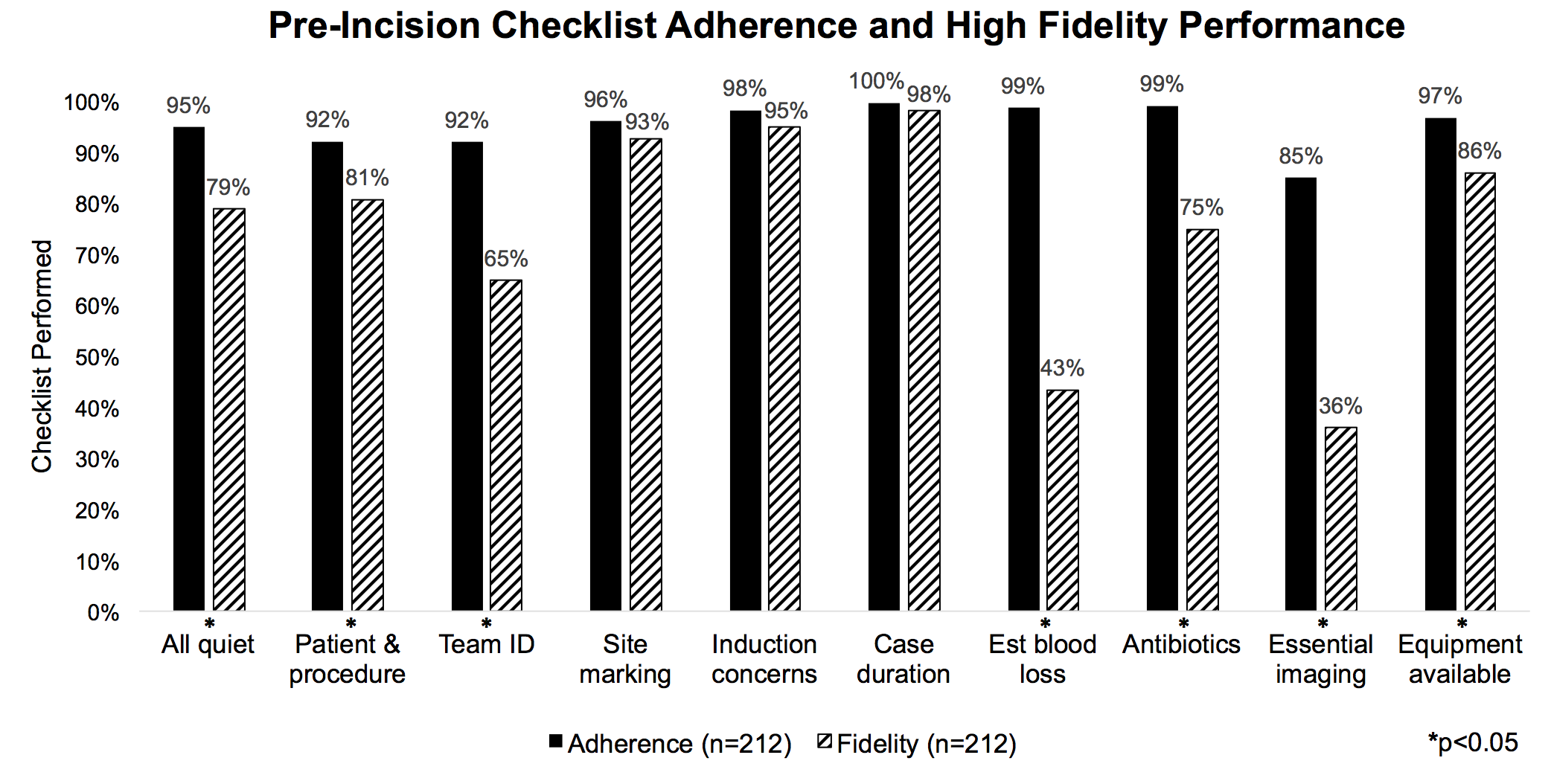
Results: 212 pediatric operations were observed representing 35 surgeons and 9 surgical subspecialties. At least one phase of the SSC was conducted in 100% of cases. 174 pre-induction, 212 pre-incision, and 199 debrief checklists were evaluated with an average adherence to each checklist of 56%, 95%, and 76%, respectively. For the pre-incision phase, adherence to checkpoint completion ranged from 85-100% and averaged 95%, yet high fidelity performance ranged from 36-98% and averaged 75%. Three pre-incision checkpoints (induction concerns, anticipated case duration, and site marking) were performed most consistently with associated meaningful completion. However, 7 checkpoints were performed at a high frequency (range 85-99%) but had a significantly lower rate of fidelity (range 36-86%, p<0.05). Inter-rater reliability kappa values for pre-induction, pre-incision, and debriefing were 0.68, 0.70, and 0.89, respectively.
Conclusion: Although surgical safety checklists are routinely performed, meaningful execution of each and every step remains suboptimal. Monitoring of implementation fidelity can identify specific processes and checkpoints upon which to focus improvement efforts.