R. S. Morris1, T. W. Yen1, A. A. Carr1, S. D. Wilson1, D. B. Evans1, T. S. Wang1 1Medical College Of Wisconsin,Surgical Oncology,Milwaukee, WI, USA
Introduction: The number of endocrine procedures, specifically parathyroidectomy, thyroidectomy, and adrenalectomy, being performed in the United States is increasing.There is a paucity of literature on the feasibility of combining these procedures in patients who may have indications for other surgical procedures.Therefore, the aim of this study was to determine the effect of performing concurrent surgical procedures on postoperative outcomes.
Methods: This is a retrospective review of multiple prospective databases of 2,930 patients who underwent thyroidectomy, parathyroidectomy, and/or adrenalectomy in combination with another procedure, at a single institution. The other procedures included skin, soft tissue, breast or hernia (SSB), abdominal major, abdominal minor, cervical, and ‘Other’. Patient demographics, operative details, and 30-day outcomes were reviewed. ‘Endocrine-specific’ complications included recurrent laryngeal nerve [RLN] injury, hypoparathyroidism, cervical wound infection, hematoma and other. ‘General’ complications included pulmonary or cardiac events and/or complications related specifically to the concurrent procedure.
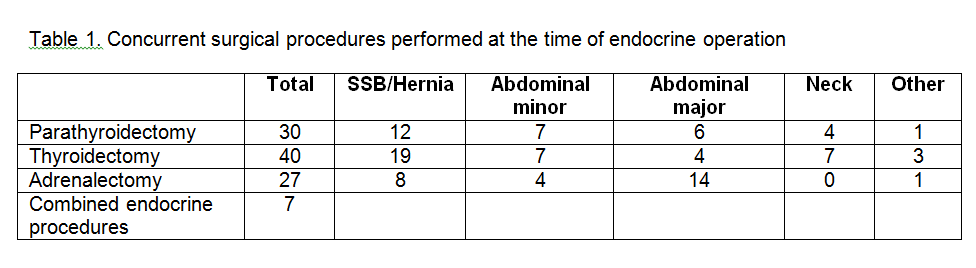
Results:The cohort is comprised of 104 patients (Table 1). Patients were managed by two surgical specialties (general surgery and an additional specialty such as orthopedics, neurosurgery or otolaryngology) in 25 (24%) patients and more than one surgeon in 57 (55%) patients. Overall, 19 (18%) patients had 21 complications, including endocrine-specific complications in eleven (11%) patients. These eleven complications included RLN injury (n=3; 3%), hematoma (n=2; 2%), wound infection (n=1; 1%), transient hypoparathyroidism (n=2; 2%) and other (n=3; 3%). One patient with hypoparathyroidism was treated with oral calcium supplementation; the other patient had a concurrent pancreatectomy and was managed with IV calcium until tolerating an oral diet. The remaining nine ‘general’ complications included pneumonia in a patient who also had RLN injury, postoperative arrhythmia in a patient who also had an additional complication, and six (6%) patients with complications specifically related to the concurrent procedure. The last patient underwent an open adrenalectomy and hysterectomy and developed a midline wound dehiscence, which could not be specifically attributed to either procedure.
Conclusion:This is a review of 104 patients undergoing a surgical endocrine procedure who underwent a concurrent surgical procedure, ranging from skin and soft tissue to major abdominal procedures. Short-term endocrine-specific complications were managed safely, suggesting that concurrent procedures can be considered, when needed, with minimal effect on patient outcomes.