G. J. Bundley1, S. K. Geevarghese2 1Meharry Medical College,School Of Medicine,Nashville, TN, USA 2Vanderbilt University Medical Center,Liver Transplant,Nashville, TN, USA
Introduction:
Resection is an important therapeutic modality for benign and malignant disease of the liver. Volumetric analysis of the liver in addition to standard assessment of patient performance status and liver function can help determine the ideal treatment plan for patients with risk factors for postoperative liver insufficiency such as cirrhosis and hepatic steatosis. Analysis using Pathfinder Scout,™ which utilizes contrasted CT or MRI data, can provide accurate future liver remnant (FLR) volume and guide assessment of resectability.
Methods:
Between 2009 and 2015, 50 patients at Vanderbilt University Medical Center were evaluated for liver resection using Pathfinder Scout™. After approval by the Institutional Review Board, the medical record of each patient was reviewed for pertinent clinical information. Data extracted from the records included preoperative diagnosis, laboratory data, type of resection planned, final pathological findings, and postoperative complications such as liver insufficiency.
Results:
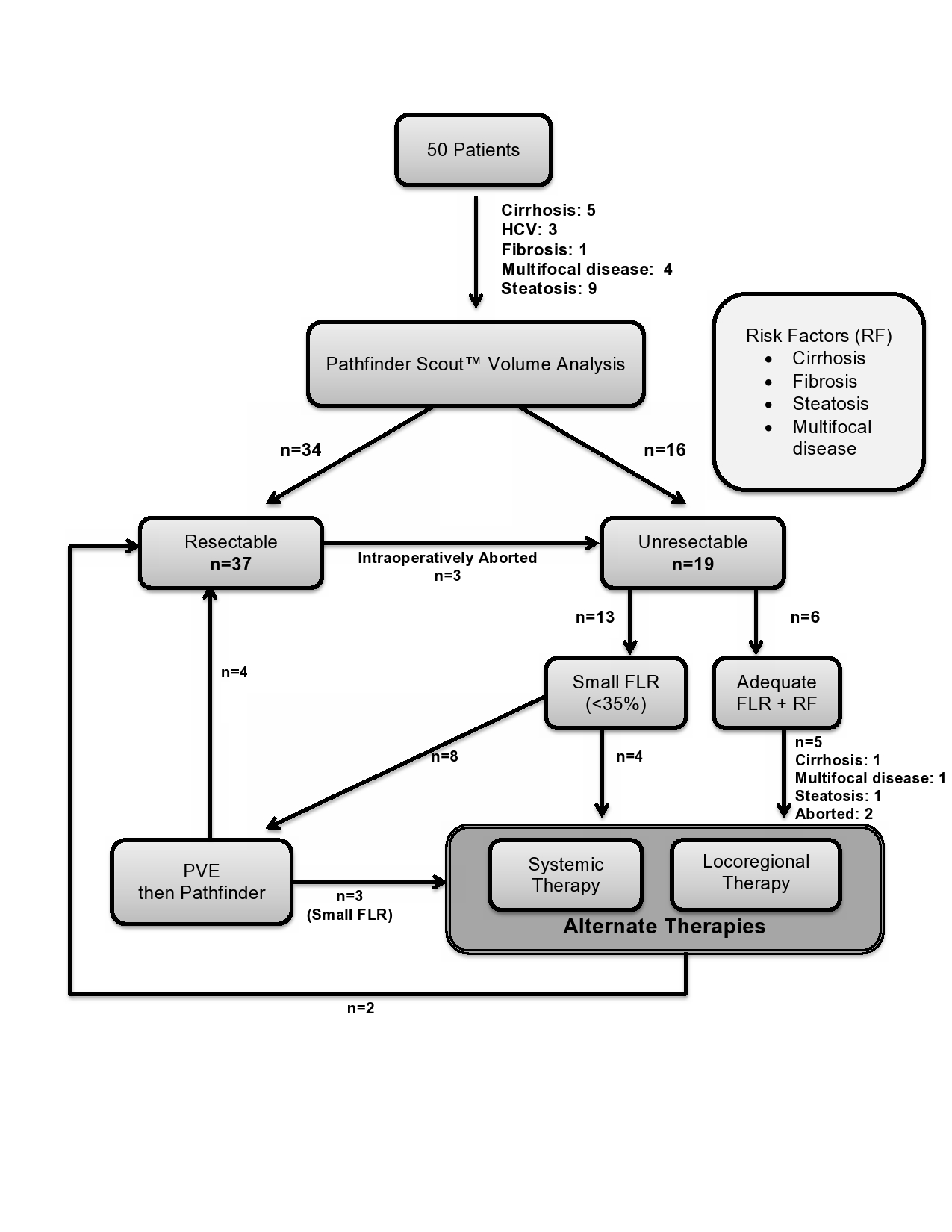
Optimal candidates for liver resection were defined as good performance status, FLR>35%, and limited risk factors. Risk factors for liver insufficiency were defined as hepatic steatosis by imaging or biopsy, fibrosis, or cirrhosis. Sixteen patients were deemed unresectable based on FLR < 35% (n=12) or adequate FLR but possessed one or more risk factors (n=4). An additional 3 resections were intraoperatively aborted due to vascular invasion or additional lesions. Four of the unresectable patients underwent locoregional therapy (LRT e.g. radiofrequency ablation, chemoembolization, radioembolization) and/or systemic therapy; two of the patients were rendered resectable. Eight patients underwent portal vein embolization (PVE) and 4 patients’ FLR improved above 35% leading to resection.
Conclusion:
Formal volumetric assessment prior to liver resection is an important consideration for patients with cirrhosis, steatosis, and multifocal disease. Based on volumetric data 24 % of patients in our cohort underwent LRT rather than resection, mitigating the risks of liver failure postresection in these patients. In addition to standard assessment of liver function and performance status, volumetric analysis of the FLR can determine the success of PVE as an adjunct to improve FLR.