K. T. Anderson1,2, L. R. Putnam1,2, T. Ostovar-Kermani1,2, E. Hamilton1,2, D. H. Pham1,2, M. T. Austin1,2, A. L. Kawaguchi1,2, L. S. Kao3, K. P. Lally1,2, K. Tsao1,2 2University Of Texas Health Science Center At Houston,Pediatric Surgery,Houston, TX, USA 3University Of Texas Health Science Center At Houston,General Surgery,Houston, TX, USA 1Children’s Memorial Hermann Hospital,Pediatric Surgery,Houston, TX, USA
Introduction: Growing concerns regarding radiation exposure in children has led to recommendations to minimize CT imaging, especially in pediatric appendicitis. However, these practices are not always adopted by non-pediatric specialties. We hypothesized that within a metropolitan hospital system (one children’s hospital (CH) and eight non-children’s hospitals (NCHs)), use of pre-operative CT is much higher in NCHs. We aimed to determine differences in pre-operative imaging and any associated demographic variables.
Methods: A retrospective study of patients <18 years undergoing appendectomy for acute appendicitis from April 2012 to April 2015 in a 9-hospital system was conducted. Patient demographics, pre-operative location, and imaging modality (computed tomography (CT) and ultrasound (US)) were evaluated. Patients were attributed to the hospital in which the pre-operative imaging was performed and not the location of appendectomy. Chi-squared, Student’s t-test, and multivariate regression were performed; p<0.05 was significant.
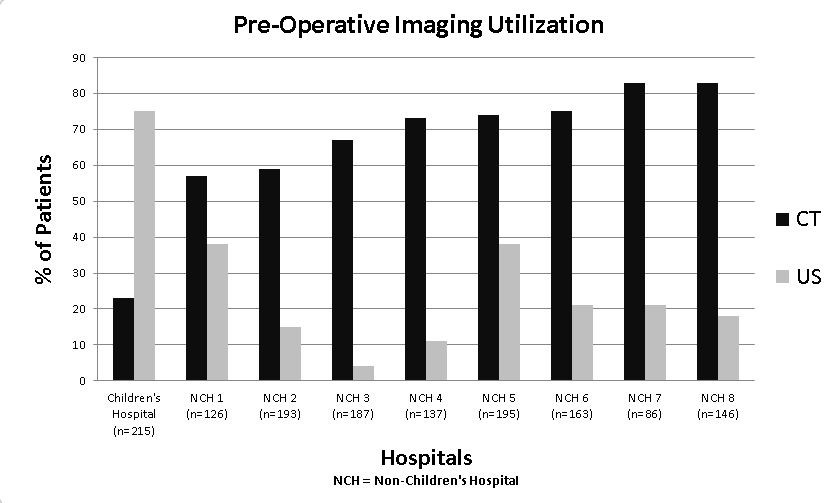
Results: 1448 pediatric patients were identified (CH=215, 15%; NCHs=1233, 85%). The median (range) number of patients triaged per NCH was 154 (85-193). Children seen at the CH were younger (mean 10.2 ± 4.0 vs 12.2 ± 3.9, p<0.01), more likely non-white Hispanic (68% vs 46%, p<0.01), and publically insured (58% vs 49%, p=0.04). CH patients underwent significantly fewer CT scans (23% vs 70%, p<0.01) and more US (75% vs 20%, p<0.01). For all patients, on multivariate regression, increased preoperative CT use was significantly associated with NCHs (OR 7.5, 95%CI 5.3-10.6), older age (age >10: OR 2.3, 95%CI 1.8-2.9), and female gender (OR 1.34, 95%CI 1.05-1.71). For patients triaged at NCHs, older age (age >10: OR 2.4, 95%CI 1.8-3.1) and female gender (OR 1.33, 95%CI 1.02-1.73) remained significantly associated with CT use. No patient characteristics were associated with increased CT use at CH. Children presenting at CH were more likely to undergo US (OR 11.8, 95%CI 8.3-16.9). Younger age (age ≤ 10: OR 1.9, 95%CI 1.5-2.5) and female gender (OR 1.5, 95%CI 1.1-1.9) were predictive of US use overall.
Conclusions: Within our hospital system, there are significant differences in utilization of imaging modalities for suspected pediatric appendicitis between CH and NCHs. Pediatric patients are 7.5 times more likely to receive a CT scan if initially evaluated in NCHs. Further investigation is needed to identify other factors contributing to imaging preference in the pediatric population in order to establish clinical practice guidelines to reduce radiation exposure in children.