B. P. Blackwood1,2, C. J. Hunter1, H. Sparks1, M. Browne3 1Ann And Robert H. Lurie Children’s Hospital Of Chicago,Pediatric Surgery,Chicago, IL, USA 2Rush University Medical Center,General Surgery,Chicago, ILLINOIS, USA 3Children’s Hospital, Lehigh Valley Health Network,Pediatric Surgery And Urology,Allentown, PA, USA
Introduction: Benign teratomas account for 80% of all teratomas. Surgical resection remains the standard of care. However, evidence-based recommendations for post-operative follow up are lacking. In some centers, patients may receive no long term follow up; whereas at others institutions, long-term care for several years may be provided. Our aim was to review outcomes of patients that have undergone therapy for benign teratomas in an effort to generate a decision tree for the follow up of these patients.
Methods: After IRB approval, the electronic medical records of patients at the Lurie Children's Hospital of Chicago (January 1st, 2005 to January 1st, 2015) were queried. Patient age, sex, classification of teratoma, surgical procedure, alpha fetoprotein levels (AFP), pathology, follow up plan, follow up time, and recurrences were recorded. Patients with the pathological diagnosis of sacrococcygeal teratoma were excluded. Statistical analysis was completed with Student’s T-test and ANOVA using Graph Pad Prism 6 software.
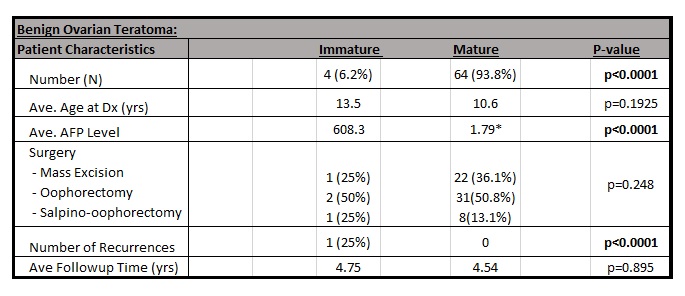
Results:We identified 73 patients with a pathologic diagnosis of a teratoma. Of these, there were 65 ovarian teratomas (4 immature, 61 mature), 5 mediastinal teratomas (all mature), and 3 retroperitoneal (1 immature, 2 mature). Ages ranged from 2 days to 21 years. There was a significant difference in the initial AFP level between the groups. The immature teratomas had an average AFP of 2239.2 and the mature teratomas had an average AFP of 3.15 (p<0.0004). There were no significant differences in follow-up time (p=0.895). There was one recurrence in the immature group and no recurrences in the mature group (p=0.0001). Overall, there was a 1.3% recurrence rate. The only recurrence was that of an immature ovarian teratoma with an initially elevated AFP of 1978. Post-operative AFP levels were not elevated, even during episodes of recurrence. We identified high variability in the recommended follow up (10 different strategies). Most commonly, an ultrasound and AFP every 3 months for 1 year, every 6 months for the next 2 years, and then yearly till 5 years postoperatively.
Conclusion:Our data indicates that patients with a diagnosis of ovarian, mediastinal, or retroperitoneal teratoma are at a low risk of recurrence after complete surgical resection. Our findings correlate with current literature in that immature teratomas may have an increased risk of recurrence as compared to the mature teratomas. Based on our review, patients with mature teratomas do not need to be followed past the initial post-operative period. However, surgeons may consider following patients with benign teratomas with immature elements, especially patients with elevated preoperative AFP, for at least one year post-operatively.