B. P. Blackwood1,2, F. Hebal1, C. J. Hunter1,3 1Ann And Robert H. Lurie Children’s Hospital Of Chicago,Pediatric Surgery,Chicago, IL, USA 2Rush University Medical Center,General Surgery,Chicago, IL, USA 3Northwestern University Feinberg School Of Medicine,Pediatrics,Chicago, IL, USA
Introduction: Intussusception is a potentially life-threatening condition and is the most frequent cause of bowel obstruction in the first two years of life. Multiple attempts at reduction are sometimes required, however intussusceptions are successfully treated with therapeutic enemas in 75-90% of cases. We hypothesized that patients who transferred from outside community hospitals (OSH) to a large academic children’s hospital with intussusception were more likely to require operative management for their intussusception than those who were directly admitted.
Methods: After IRB approval the electronic medical record was queried for patients presenting to Ann and Robert H. Lurie Children's Hospital of Chicago with a diagnosis of intussusception (July 1st, 2009 – July 1st, 2014). Age, sex, symptom duration, radiologic management, and surgical care were recorded. Additionally, OSH and transfer reports were analyzed for those patients that presented as a transfer. Statistical analysis was performed with Student’s T-test and ANOVA using Graph Pad Prism 6 Software.
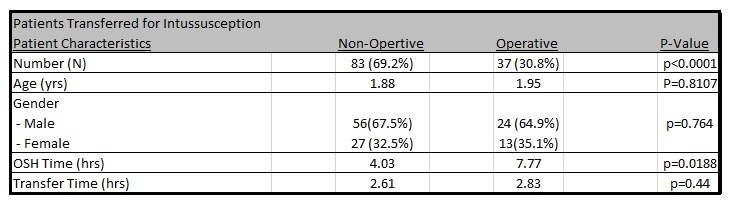
Results:We identified 270 patients with intussusception confirmed radiographically with ultrasound or CT. Of these patients, 212 (78.5%) were successfully treated non-surgically, and 58 (21.5%) required surgical management. Of the patients requiring surgery, there were 38 reductions (24 laparoscopic, 14 open) and 20 bowel resections (1 laparoscopic, 19 open).There were 120 (47.2%) transfers from OSH. Of those patients requiring surgery, 37 (63.8%) had presented as a transfer from an OSH. We found that transferred patients, requiring surgery, spent a mean 7.77 hours at the OSH compared to 4.03 hours for the transferred patients that did not require surgery (p=0.0188). There was no significant difference in transport time (p=0.44).
Conclusion:In conclusion, intussusception can be managed non-operatively 78.5% of the time based on our experience. We have identified the amount of time patients spend at hospitals without pediatric surgical capabilities as an independent risk factor necessitating surgical management of intussusception. These data suggest that patients with the diagnosis of intussusception who present to hospitals without pediatric radiology or pediatric surgery, should be transferred in an expedited fashion. Furthermore, in the event of a failed enema reduction at an OSH the transport of the patient should not be delayed as this may result in a higher likelihood of surgical management.