A. Adkins2, U. Pandya1 1Grant Medical Center,Trauma Services,Columbus, OH, USA 2The Ohio State University,College Of Medicine,Columbus, OH, USA
Introduction: Extubation failure and subsequent reintubation is associated with longer intensive care unit and hospital stay and worse outcomes when compared to successfully extubated patients. For many institutions, a successful spontaneous breathing trial is the primary criteria to determine readiness for extubation. Patients with traumatic injury, however, represent a unique population that requires special consideration. It seems reasonable that injury types such as rib fractures and cervical fractures could influence success of extubation. Relatively few studies on this topic have focused on the trauma patient population and their specific injury types. The purpose of this investigation is to determine if specific types of traumatic injury predispose patients to extubation failure. We hypothesize that rib fractures and cervical spine fractures are risk factors for failed extubation despite having a successful spontaneous breathing trial.
Methods: This study was a retrospective chart review of all trauma patients admitted to Grant Medical Center over a 6 year period from January 2009 to December 2014. All injured patients on mechanical ventilation over the age of 15 were considered for the study. Patients that were endotracheally intubated and subsequently passed a spontaneous breathing trial were included. Exclusion criteria were self-extubation, tracheostomy placement prior to attempted extubation, palliative withdrawal of life support, or death prior to an extubation attempt. Patients requiring re-intubation within 72 hours of extubation were determined to have failed extubation and were compared to patients who had successful extubation. Differences between the two groups were analyzed with a p value < 0.05 signifying statistical significance. Multiple regression analysis was used to control for age, injury severity score, and vent days prior to extubation.
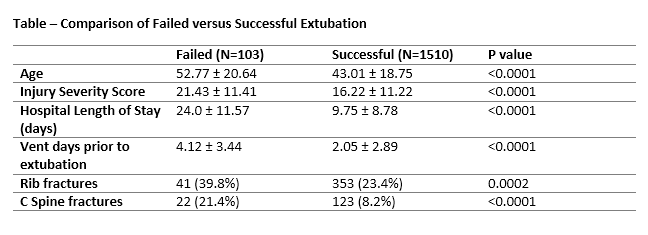
Results: A total of 1,613 patients met inclusion criteria with 103 (6.4%) of those in the failed extubation group. Patients who failed extubation were older, had higher injury severity score, more ventilator days prior to extubation, and more intensive care unit and hospital days. Patients who failed extubation were more likely to have cervical spine fractures (21.4% versus 8.2%, p = <0.0001) and more likely to have rib fractures (39.8% versus 23.4%, p = 0.0002).
Conclusion: Cervical spine fractures and rib fractures are risk factors predictive of failed extubation despite successful spontaneous breathing trial. These patients may require additional weaning criteria to better determine chances of successful liberation from mechanical ventilation.