J. Pattison2, U. Pandya1 1Grant Medical Center,Trauma Services,Columbus, OH, USA 2Ohio University College Of Osteopathic Medicine,Heritage College Of Osteopathic Medicine,Athens, OH, USA
Introduction: Dysphagia is a common condition in the elderly with significant complications such as aspiration, pneumonia, and potentially increased mortality. This problem is even more magnified in elderly patients with cervical spine fractures as neck positioning and altered physiology may further predispose these patients to complications. Fractures of the cervical spine can span the entire length of the neck from C1 to C7. It stands to reason that injuries at different levels of the cervical spine could influence swallowing function in unique ways. This study seeks to investigate how the level of cervical fracture in elderly patients who are non-operatively managed impacts the incidence of dysphagia.
Methods: Medical records of all trauma patients age 65 and older admitted with cervical fractures between January 2008 and April 2014 to a level 1 trauma center were retrospectively reviewed. Patients with a past medical history of dysphagia or stroke or who had operatively managed fractures were excluded, leaving 123 patients for analysis. Bedside evaluation of swallowing function was performed and any patients with evidence of swallowing dysfunction had formal speech therapy consultation. Dysphagia was defined as any restriction or diet modification as a result of swallowing dysfunction after speech therapy assessment. Demographic data, hospital length of stay, intensive care unit days, ventilator days, injury severity score, mortality and level of cervical fracture were analyzed. P values < 0.05 were considered statistically significant. Multiple regression analysis was used to control for confounding variables.
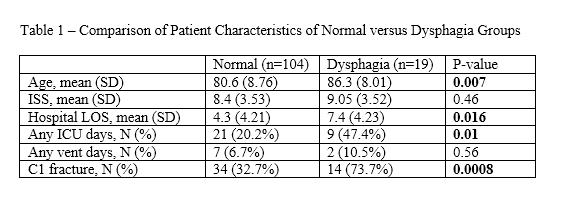
Results: A total of 123 patients met inclusion criteria and 19 (15.4%) of those patients had dysphagia Patients with dysphagia were older (86.3 ± 8.01 vs. 80.6 ± 8.76, p = 0.007), had higher hospital length of stay (7.4 ±4.23 vs 4.3 ± 4.21, p = 0.016), and were more likely to have intensive care unit days (47.4% vs 20.2%, p=0.01).. Patients with C1 fractures were more likely to have dysphagia than patients with other cervical fractures (29.2% vs 7.1%, p = 0.0008). After using regression analysis to control for total length of stay, any intensive care unit days, and age, C1 fracture increased the likelihood of dysphagia by 4 times (OR = 4.0; 95% CI 1.2-13.0)
Conclusion: Incidence of dysphagia is significant in geriatric trauma patients with cervical spine fractures and has important ramifications for patient outcomes such as hospital length of stay. Patients with C1 fractures are at increased risk for dysphagia and these patients may benefit from more vigorous surveillance to prevent subsequent complications.