E. Eklund1, O. Kassar1, N. Napoli2, W. Barnhardt3, L. Barnes2, J. Young1 1University Of Virginia,Department Of Surgery,Charlottesville, VA, USA 2University Of Virginia,Department Of Systems & Information Engineering,Charlottesville, VA, USA 3University Of Virginia,Emergency Services,Charlottesville, VA, USA
Introduction: During mortality gap analysis using our Relative Mortality Metric (RMM) of patient populations separated by Abbreviated Injury Scale-coded regions obtained from our institutional trauma registry, it could be seen that there was little difference in relative mortality between single and multiple injury. Therefore we examined trauma populations to determine whether patients demonstrated statistically significant differences in mortality under mono- and polytrauma conditions.
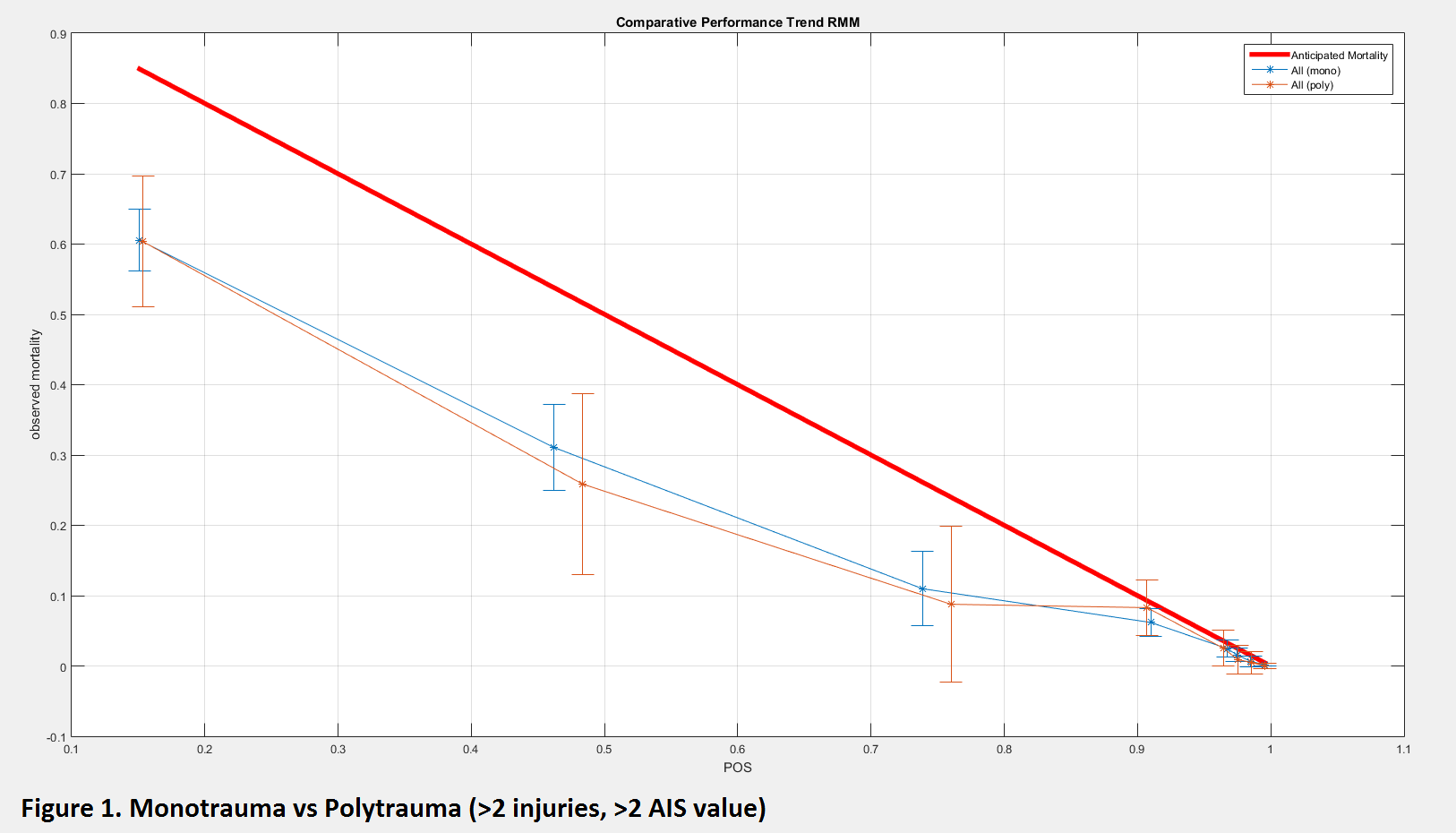
Methods: We examined data from an initial population of 38000 patient encounters from 1994 to present, yielding a final sample size of approximately 25000. Raw data were cleaned and analyzed using our RMM that describes the overall performance in relation to the anticipated mortality (benchmark TRISS threshold) and observed mortality, where RMM has a range from -1 to 1. Monotrauma (n=8606) and polytrauma (n=16250) were analyzed (defined as a single or multiple AIS-coded injuries in the registry). The relation was further evaluated by stratifying patients into subpopulations based on their overall number of injuries (1, 2-5, 6-10, and 11+) and evaluating mortality differences. Additionally, a second polytrauma definition (>2 injuries with AIS score >2) was used to assess whether patient group mortality differences held. Finally, head monotrauma was separated from the rest of the monotrauma patient population in order to determine if single high mortality head injuries could be driving monotrauma toward greater expected mortality.
Results: When each population was plotted across all AIS values and regions, no significant difference in RMM value between mono- and polytrauma was found (RMM values of 0.3392 and 0.3576, respectively) and each curve fell within the 95% confidence interval of the other. Furthermore, when data was divided by AIS region, the two largest groups (head+face and extremity) mirrored the overall trends. Subsequent analysis of injury number-stratified polytrauma subpopulations again showed no significant difference between mono- and polytrauma. Lastly, when head monotrauma was separated from the rest of the monotrauma population, there was again no significant shift of the curve toward increased patient survival relative to the polytrauma population.
Conclusion: We hypothesized that polytrauma would result in increased mortality due to the compounding effects of multiple sites of injury. However, it was seen that there is no notable difference in the mortality gap as defined by RMM value between different anatomical sites when comparing mono- and polytrauma. This trend held even when confounding factors such as differing levels of polytrauma and the sometimes more severe nature of singular head injuries were controlled for.