H. Shi2, M. Esquivel1, K. Staudenmayer1, D. Spain1 1Stanford University,Department Of Surgery,Palo Alto, CA, USA 2Case Western Reserve University School Of Medicine,Cleveland, OH, USA
Introduction: Rib fractures are the most common type of chest trauma sustained by elderly patients and are often associated with significant morbidity and mortality in this patient population. Based on studies that show 2-5 times the mortality in patients ≥ 65 with 2 or more rib fractures, our academic institution and Level I trauma center recommends intensive care unit (ICU) admission for the first 24 hours. In this study, we aim to evaluate the utilization of the protocol and outcomes of this patient population.
Methods: A retrospective review was completed of all patients ≥ 65 years of age in our Trauma Registry who sustained isolated rib fractures from January, 2008 to March, 2015 at an urban Level I Trauma center. Data included basic demographics, comorbidities, injuries, length of intensive care unit and hospital stay (LOS), ventilator days, analgesic used, morbidity, mortality and disposition.
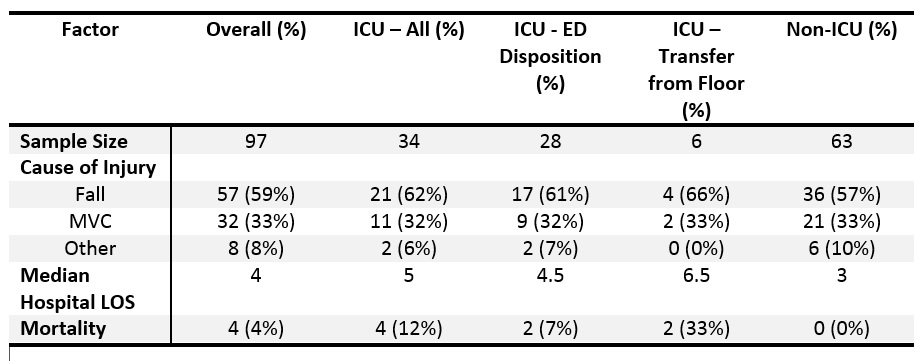
Results: Over the 7 year period, a total of 97 patients ≥ 65 years of age with at least one rib fracture and an Abbreviated Injury Score (AIS) of < 2 for other regions were admitted. The median age of these patients was 80 years, 55% were female, and 90% had two or more rib fractures. Fall was the cause of 58% of injuries, while motor vehicle collision (MVC) accounted for 33%. Of the 87 patients with more than one rib fracture, 69 (71%) were not admitted directly to the ICU and 6 (9%) of those were subsequently transferred to the ICU with a mortality of 2.9% for patients with ≥2 rib fractures not admitted directly to the ICU. Of the 4 (4%) mortalities, 3 were caused by falls and 1 by MVC. Patients who fell had a median hospital LOS that was 0.5 to 1 day longer than patients who suffered other mechanisms of injury or were involved in a MVC respectively. Patients aged 70 or older had a median length of stay of 4 days, twice the median length of stay for those between 65 to 69 years old.
Conclusion: With an aging population, trauma in the elderly will continue to increase, likely with a high volume of rib fractures. It is critical to understand the best course of triage and management for this high risk population. We found that falls were the most common mechanism of injury and had the highest median LOS and median number of rib fractures. We also found that patients over the age of 70 had a longer median LOS than those younger and admitting all patients ≥ 65 years of age is likely not necessary, though further research is needed to determine more discrete age and fracture cut-offs.