N. Dagher1, I. Olorundare1, S. DiBrito1, C. Landzabal1, D. Segev1,2 2Johns Hopkins Bloomberg School Of Public Health,Department Of Epidemiology,Baltimore, MD, USA 1Johns Hopkins University School Of Medicine,Department Of Surgery,Baltimore, MD, USA
Introduction: Published case series and opinion articles have suggested that kidney transplant recipients (KTR) have higher complication rates and longer length of stay (LOS) following appendectomy than non-transplant patients (NTP). Literature suggests that compared to laparoscopic appendectomy (LA), open appendectomy (OA) is safer, associated with fewer complications in KTR. Those assumptions have likely resulted in a shift of KTR care from the community to kidney transplant (KT) centers and to a conservative open approach. This is the only reported study to date investigating outcomes of LA vs OA in the KTR population using a large nationwide dataset.
Methods: The Nationwide Inpatient Sample database was used to identify 1336 KTR and 2.6 million NTP who underwent appendectomy between 2000-11. Surgical approach (LA vs OA), and location of surgery at either a transplant center (defined as a hospital performing at least one KT during the study period) or a non-transplant center were compared. Postoperative complications for both groups were categorized using ICD-9 codes and risk factors for complications were tested using logistic regression. Negative binomial regression models were used to compare LOS and hospital charges.
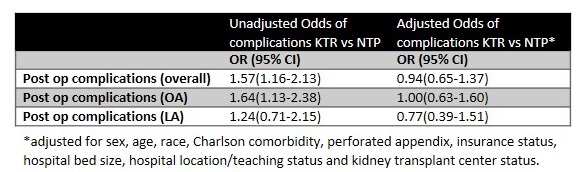
Results: A total of 1336 KTR and 2.6 million NTP who underwent appendectomy were identified. LA was performed in 44% of KTR and 55% of NTP. KT centers performed 49.6%(663) and non-KT centers performed 50.4%(673) appendectomies on KTR. Although the overall rate of complications in KTR was significantly higher than in NTP undergoing OA (22.2% vs 14.8%), they were similar for LA (10.6% vs 8.7%). Compared to NTP, KTR were not at greater risk of complications overall (OR 0.95, 95% CI: 0.65-1.37). However, they were more likely to have infectious (OR: 1.82, 95% CI: 1.00-3.31) or wound (OR 3.25, 95% CI: 1.41-7.48) complications. Median LOS was longer in KTR regardless of surgical approach (KTR: 3 days for LA vs 4 days for OA; NTP: 2 days for LA vs 3 days for OA). Median hospital costs were higher for KTR for both LA and OA ($8600 and $9900 for KTR vs $7100 and $6300 for NTP). Transplant centers and non-transplant centers had similar complication rates (14.8% vs 19.2%), LOS (median 3 vs 3 days), and hospital charges ($6700 vs $6800) for KTR.
Conclusion: Though KTR are more likely to have an OA, they have better outcomes following LA and are comparable to NTP. This suggests that when indicated and technically feasible, LA should be favored. KTR have a longer LOS and higher hospital charge regardless of surgical approach or type of center. Outcomes do not differ significantly between transplant and non-transplant centers suggesting it is safe to perform appendectomy on KTR at either type of center.