E. A. Pomfret1, M. Akoad1, M. Simpson1, J. J. Pomposelli1 1Lahey Hospital And Medical Center,Transplantation And Hepatobiliary Diseases,Burlington, MA, USA
Introduction: Despite widespread success, there is still debate regarding the appropriate timing of LDLT. Patients with high MELD scores are often considered too sick for LDLT while those with low MELD scores may be considered ‘too early’. We compared characteristics of LDLT recipients with those patients without LDs who died on the waiting list during the same time period. The purpose of the study was to determine if patients with end-stage liver disease and availability of a LD are less likely to die on the waitlist.
Methods: Demographic and clinical data of patients who received LDLT (LD) or who died on the waitlist (DOW) between 2002 and 2013 were compared. Statistical analysis was performed sing SPSS; p values <0.05 were considered significant.
Results: 204 LDLT recipients and 198 patients who DOW were identified. Both groups were male predominant (72% LD vs. 62% DOW) and had similar MELD scores at evaluation (14.1+6.0 LD vs.15.7+6.5 DOW). Patients who died while waiting had lower platelet counts (105 vs. 149 LD, p=0.009) and albumin (2.6 vs. 3.2 LD, p=0.01) at evaluation and higher incidence of SBP (43.3% vs. 26.9% LD, p=0.001) than patients with LD. Their MELD at death was 24.9+12.9 vs. 14.8+6.0 at LDLT (p=0.001). Mean platelet count at death was 70.1 vs.136 at LDLT (p=0.002).
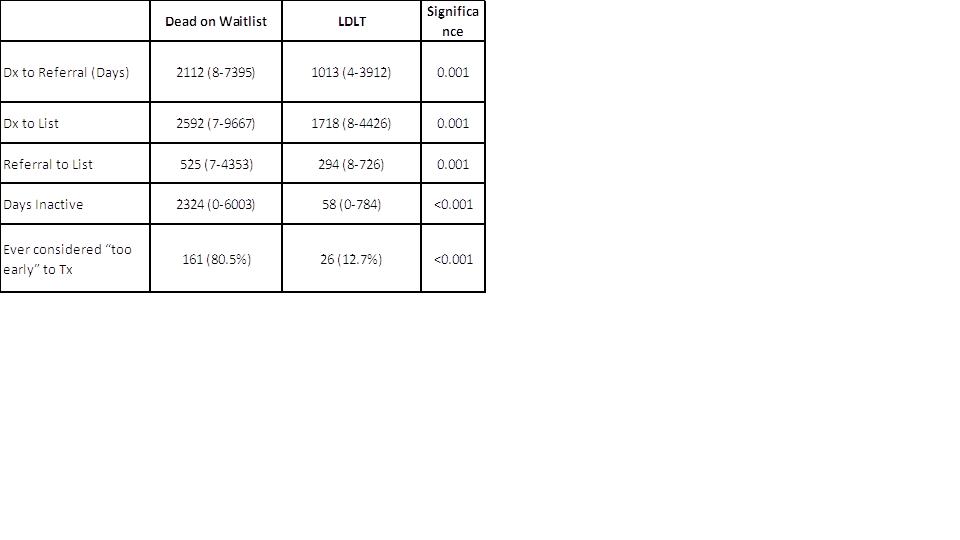
Additional comparisons are shown in Table 1.
Conclusion: Patient with an available LD are referred, listed and transplanted significantly earlier that those waiting for a deceased donor. Despite similar initial MELD scores, patients with LD were transplanted with improved nutritional status, less portal hypertension, fewer decompensating events such as spontaneous bacterial peritonitis (SBP) and were less likely to be temporarily inactivated. Availability of a LD affords the recipient with end-stage liver disease rapid referral, higher transplant rates, and less morbidity and mortality prior to transplant. Labeling candidates as ‘too early’ based on MELD score increases days inactivated and may result in worse outcomes.