K. Bittner1, M. C. Mora1, K. Douglas1, K. Wong1, D. Tashjian2, K. Moriarty2, M. Tirabassi2 1Baystate Medical Center,Springfield, MA, USA 2Baystate Children’s Hospital,Springfield, MA, USA
Introduction:
Blood loss is an important factor affecting perioperative outcomes in patients undergoing ex-situ split liver transplantation. The purpose of this study was to determine if monopolar electrocautery can be used to achieve hemostasis in an ex-situ liver transection model.
Methods:
Following euthanasia of Yorkshire swine utilized from an IACUC-approved study, a midline laparotomy was performed. The left hepatic lobe was incised twice to length 6cm and depth 1cm utilizing either monopolar electrocautery (in-situ cautery, ISC) or a 10 blade (in-situ knife, ISK). For ISC, the animal was grounded using a standard adhesive grounding pad. Vascular inflow and outflow to the liver was controlled. The liver was then perfused with heparinized ice-cold lactated ringers. Next, the liver was harvested, transferred to a sterile back table, and placed into a container containing slush solution. The container was set on a draped reusable non-contact grounding electrode pad. Ex-situ, the liver was incised with monopolar electrocautery (ex-situ cautery, ESC) and was then re-perfused with heparinized whole pig blood (203±129mL/pig). After re-perfusion, total blood loss from each liver parenchymal incision was quantified by weight via capture into absorptive gauze. Hematoxylin and eosin (H&E), and fluorescent staining with Phalloidin (F-actin) on liver samples were performed to compare the effects of ISC and ESC.
Results:
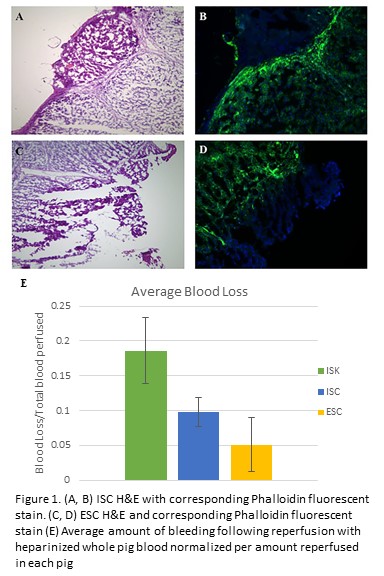
In all three re-perfused pig livers, ISK demonstrated the greatest blood loss. In 2/3 pigs, ESC resulted in less bleeding versus ISC. As each pig had a different amount of blood reperfused, data was normalized as a percentage of reperfused blood for each pig (Figure 1E). In ESC and ISC, H&E sections of livers revealed fragmented margins, cell distortion, and elongated nuclei consistent with electrocautery injury (Figure 1A&C). Staining with Phalloidin in both groups revealed a zone of denatured actin corresponding to areas of electrocautery use (Figure 1B&D).
Conclusion:
Monopolar electrocautery can effectively be performed in ex-situ liver transections using a commercially available non-contact grounding electrode pad. Incorporation of this technique in ex-situ liver procedures can potentially result in reduced blood loss after transplantation.