M. D. Ray-Zack1, Y. Shan1, P. Kerr1, C. Kosarek1, H. Hudgins1, U. Jazzar1, D. Tyler1, S. J. Freedland3, T. Swanson1, A. Kamat2, J. L. Gore4, S. Kaul1, H. Mehta1, S. B. Williams1 1The University of Texas Medical Branch,Surgery/Urology,Galveston, TX, USA 2MD Anderson Cancer Center,Urology,Houston, TX, USA 3Samuel Oschin Comprehensive Cancer Institute, Cedars-Sinai Medical Center,Surgery,Los Angeles, CA, USA 4University Of Washington,Urology,Seattle, WA, USA
Introduction:
In this study, we compared costs associated with trimodal therapy versus the guideline-recommended radical cystectomy among older adults with muscle-invasive bladder cancer.
Methods:
Using Surveillance, Epidemiology, and End Results (SEER)-Medicare linked data, we enrolled a total of 2,963 patients aged ≥66 years diagnosed with clinical stage T2-4a bladder cancer between 2002 and 2011. We compared total Medicare costs within one year of diagnosis among patients following radical cystectomy or trimodal therapy using inverse probability of treatment weighted (IPTW) propensity score models, which included a two-part estimator to account for intrinsic selection bias.
Results:
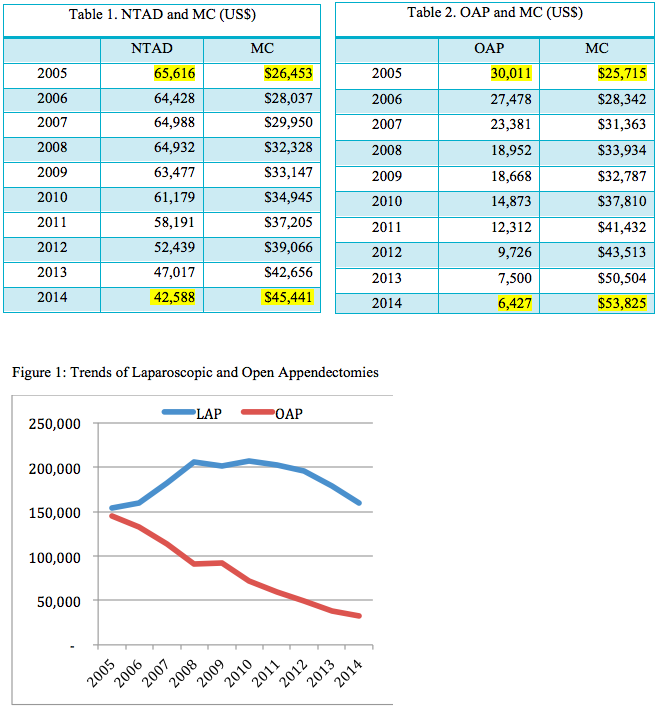
Median total costs were significantly higher for trimodal therapy than radical cystectomy in 90 days ($83,754 vs. $68,692; median difference $11,805, 95% CI $7,745 to $15,864), 180 days ($187,162 vs. $109,078; median difference $62,370, 95% CI $55,581 to $69,160), and 365 days ($289,142 vs. $148,757; median difference $109,027, 95% CI $98,692 to $119,363). Outpatient, radiology, pharmacy and pathology/laboratory costs contributed largely to the significantly higher costs associated with trimodal therapy (Figure 1). On IPTW-adjusted analyses, patients undergoing trimodal therapy had $142,337 (95% CI $117,423-$175,300) higher costs compared with radical cystectomy one year after treatment.
Conclusion:
Compared to radical cystectomy, trimodal therapy was associated with higher costs among patients with muscle-invasive bladder cancer. Extrapolating cost figures to the total US population resulted in excess spending of $853 million for trimodal therapy compared with radical cystectomy for patients diagnosed in 2018.