H. J. Hawthorne1, T. N. Cohen1, W. D. Cammon1, J. Bingener2, S. Hallbeck1, J. Kang3, P. Santrach4, S. A. Elliott5, R. C. Blocker1 1Mayo Clinic,Center For The Science Of Health Care Delivery,Rochester, MN, USA 2Mayo Clinic,Department Of Surgery,Rochester, MN, USA 3Mayo Clinic,Office Of Leadership And Organization Development,Rochester, MN, USA 4Mayo Clinic,College Of Medicine,Rochester, MN, USA 5Mayo Clinic,Department Of Nursing,Rochester, MN, USA
Introduction: To improve a common source of communication breakdown in patient care, the Institute for Healthcare Improvement published a standardized handoff communication tool known as ‘SBAR’ (Situation (S), Background (B), Assessment (A) and Recommendation (R)). This study explored the use of SBAR for handoffs between surgical team members 6 years after implementation in a large tertiary care center.
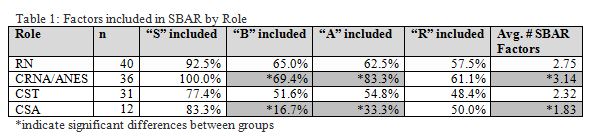
Methods: Healthcare systems engineering researchers observed 23 operative procedures in June 2015. Case duration, presence and duration of handoffs, were recorded for the following participants – circulating registered nurses (RN), certified surgical technicians (CST), certified surgical assistants (CSA), and anesthesia providers including certified registered nurse anesthetist and anesthesiologists (CRNA/ANES). To evaluate the use of SBAR during handoffs, a binary approach to determine existence or nonexistence of each SBAR component (S, B, A, R) was applied and analyzed using nonparametric statistics.
Results: Of the 23 procedures (M = 219 min, SD = 92), 20 included at least one handoff during the operative procedure. Within these 20 cases, 127 handoffs were observed of which 119 could be assessed for SBAR use. CSAs performed fewer handoffs (10%) than CSTs (26%), anesthesia providers (30%) and RNs (34%) (p=0.0014). Of the 119 handoffs (M = 61sec, SD = 52), 90% included information about the patient’s situation, 58% discussed clinical background, 64% provided an assessment and 55% made a recommendation. SBAR components included in each handoff varied significantly by the role involved; specifically differences exist between CRNA/ANES and CSAs when evaluating use of ‘B’ (p=0.032), ‘A’ (p=0.048) and average number of SBAR factors included (p=0.043). When the core team member present at the start of the case handed off, information about the situation was included in 94%, background in 69%, assessment in 68% and recommendation in 68% of handoffs. The average number of SBAR factors used differed by who provided the handoff (original →relief, relief →original, relief →relief) (p=0 .0018), driven by the use of ‘B’.
Conclusion: This pilot study suggests that in a busy OR a handoff by a team member may occur every 35 minutes and adoption of the SBAR structure during surgical procedures differs by role and situation. Team members adjusted for prior knowledge (e.g. ‘B’) by the core team. The study was not scoped to investigate the effect of surgeon briefings on the differential use of SBAR or the effect of differential use of SBAR on the occurrence of non-routine events.