A. AlKukhun1, A. Bertacco1,2, G. Caturegli1, F. D’Amico1,2, R. Morotti1, M. I. Rodriguez1, D. C. Mulligan1, J. P. Geibel1 1Yale University School Of Medicine,Surgery,New Haven, CT, USA 2Padova University,HPB And Liver Transplant,Padova, VENETO, Italy
Introduction: The small intestine remains one of the most sensitive organs to ischemic injury prior to transplantation. In the present study, we assessed in a rat model the optimal preservation temperature for intestinal grafts by comparing normothermic to hypothermic perfusion preservation.
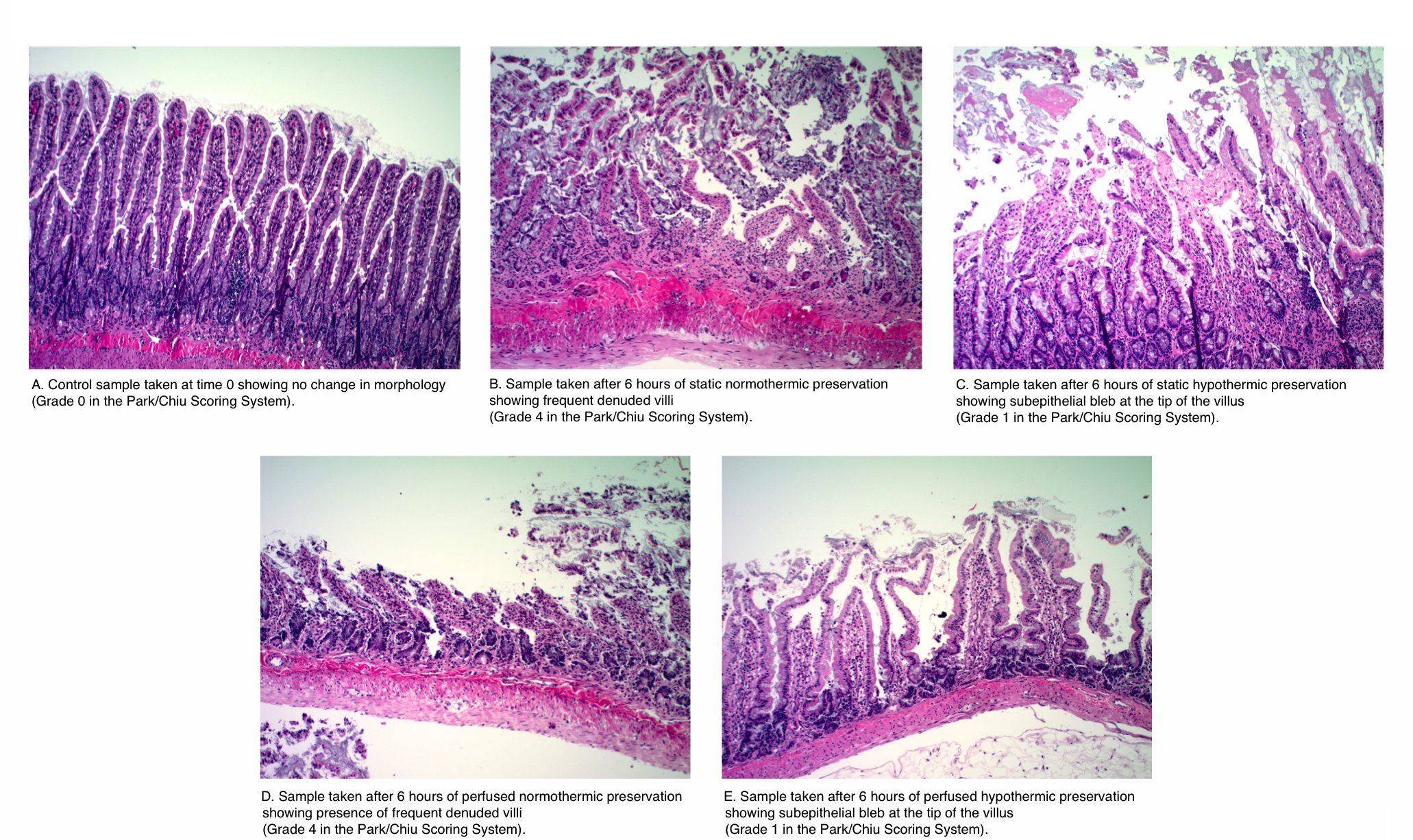
Methods: Small intestine segments were procured from rats and connected to customized chambers and a perfusion system. Paired intestinal segments were perfused in the luminal and vascular side with University of Wisconsin Solution at two different temperatures (37 and 4 Celsius) over 6 hours. Intestinal tissue samples were processed and evaluated by a blinded pathologist using the Park/Chiu Scoring System for Grading Intestinal Ischemia.
Results: The histopathological analysis showed that continuous perfusion of the intestinal segments at 4 Celsius better preserves the small intestinal segment in comparison to perfusion at 37 Celsius at 6 hours. The differences among the means (hypothermic: 1.67 vs. normothermic: 3.5) in the scoring was significant at an alpha level of 0.05 (p-value=0.0048). The attached figure displays the pathological analysis of the samples.
Conclusion: In conclusion, continuous hypothermic perfusion of small intestinal grafts with University of Wisconsin solution resulted in improved preservation of the intestinal tissue in comparison to continuous normothermic preservation. These results suggest that continuous perfusion at normothermic conditions shows no advantage to continuous hypothermic perfusion as judged by pathological evaluation.